Common Symptoms
The ABCDE warning signs help spot melanoma early.
- Asymmetry: The spot or mole has an irregular shape, with two parts that look very different.
- Border: Edges are irregular, jagged, or scalloped.
- Color: The spot has multiple colors, such as varying shades of tan, brown, or black, or patches of white, red, or blue.
- Diameter: The spot is larger than 6 millimeters across.
- Evolving: The mole or spot changes in size, shape, or color. It may also start to bleed, itch, or crust.
Melanomas can have different appearances. In addition to the ABCDE warning signs, other common signs include:
- New or Unusual Spot: A spot that looks like a new mole, freckle, or age spot, but stands out from others on your skin.
- Nodule or Sore-Like Growth: A firm, dome-shaped bump that may look like a sore and could bleed.
- Dark Line Under a Nail: A vertical brown or black streak beneath a fingernail or toenail.
- Pigmented Band Around a Nail: A darker-colored band encircling a fingernail or toenail.
- Scar-Like Patch: A slowly growing, thickened patch of skin that resembles a scar.
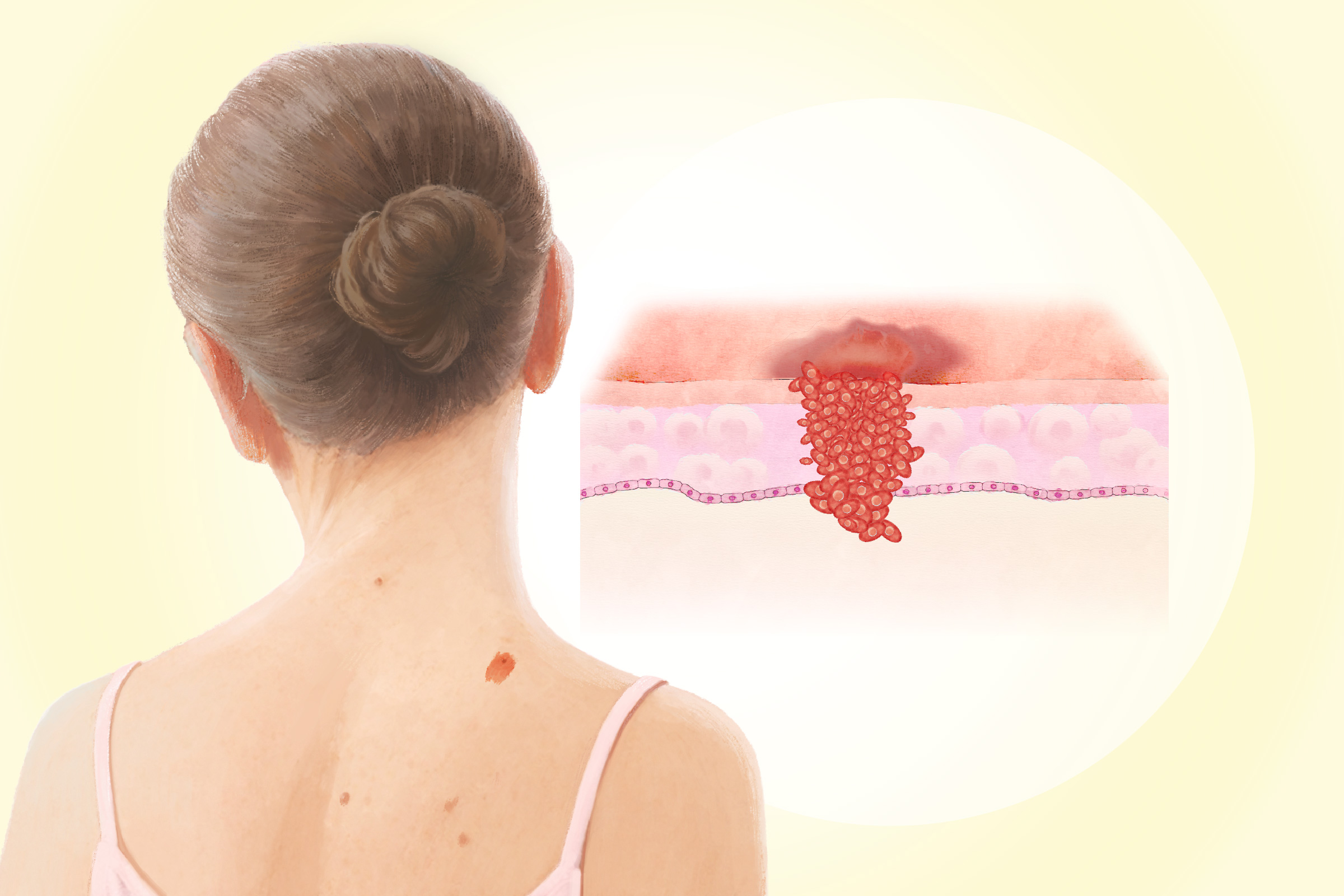
Based on appearance, growth pattern, growth rate, and location on the body, melanoma has several types. The three most common are:
- Superficial Spreading Melanoma (70 Percent of Cases): It typically appears flat and thin—less than 1 millimeter thick—with an irregular border and various colors, including red, blue, brown, black, gray, and white. It often develops from an existing mole and commonly occurs on the torso, arms, and legs.
- Nodular Melanoma (15 Percent to 20 Percent of Cases): This is one of the most aggressive types. It grows downward into the skin and appears as a raised, protruding growth, often resembling a mushroom with a stem. It typically appears black but may occasionally be red, pink, or the same color as the surrounding skin. It is commonly found on the face, chest, or back, and areas not typically exposed to the sun.
- Lentigo Maligna Melanoma (1o Percent to 15 Percent of Cases): Typically affecting older people, it often presents as a large, flat tan or brown patch with an irregular border. It gradually darkens as it grows and may display multiple shades of brown or black. Initially, it may originate from an in situ tumor called lentigo maligna, limited to the epidermis (the outer layer of the skin). This type primarily develops on sun-exposed areas such as the face, ears, and arms.
Risk Factors
Several environmental and lifestyle factors can contribute to melanoma.
- Ultraviolet (UV) Light Exposure: Sunlight has a variety of benefits: it boosts immunity, regulates circadian rhythm, helps producing vitamin D, serotonin, melatonin, nitric oxide, and even helps reduce the risk of cancers. Many people don’t get enough sunlight. However, getting too much UVB and UVA rays, including its artificial sources, can have its downside. A 2025 study found tanning bed use was associated with nearly a threefold increase in melanoma. Intense sun exposure—especially sunburns during childhood—raises risk. Children and young adults who experience intense sun exposure may not develop cancer until many years or even decades later.
- Tattoos: A 2025 study found that people with tattoos have a 29 percent higher chance of developing melanoma. When tattoo ink is injected into the skin, the immune system treats it as a foreign substance and traps the pigments in immune cells that can carry them to lymph nodes, where they may break down into potentially cancer-causing chemicals.
- Occupational Exposure to Polychlorinated Biphenyls (PCBs): PCBs are harmful chemicals used in the plastics and chemical industries. Workers exposed to PCBs may have an increased risk of developing melanoma.
- Family History: About 5 percent to 10 percent of people with melanoma have a family history of the disease. Having at least one first-degree relative—parent, sibling, or child—with melanoma more than doubles your risk. This increased risk may reflect shared skin type and sun exposure habits or, in rare cases, inherited genetic mutations.
- Moles: Most babies are born without moles, which typically appear during childhood and young adulthood. Having more than 50 moles increases melanoma risk. Atypical moles, which are larger, oddly shaped, or unevenly colored, also increase risk, although only a small percentage actually become cancerous. The highest risk comes from atypical mole syndrome, an inherited condition in which people have many atypical moles and require frequent dermatology exams and monthly self-checks. Large moles present at birth—especially those covering large areas of the back or buttocks—carry a significantly higher risk and may require surgical removal, while small congenital moles pose minimal risk.
- Light Skin, Hair, and Eye Colors: People with fair skin, light-colored hair, and blue, green, or gray eyes have a higher risk of melanoma because they have less melanin, which helps protect against UV radiation.
Melanoma risk increases with age, but it can also occur in younger people. It is one of the most common cancers in people under 30, especially young women. In families with inherited melanoma, the disease may appear at an earlier age. In addition, men are more likely than women to develop melanoma. Some evidence suggests taller people have a higher risk of melanoma.
- Genetic Disorders: Certain inherited conditions increase melanoma risk, including xeroderma pigmentosum (which prevents the skin from repairing UV damage), Werner syndrome (which causes rapid aging), and hereditary retinoblastoma (caused by an inherited gene mutation).
- Weakened Immune System: A healthy immune system helps protect against melanoma and other cancers. People with weakened immunity—due to medical conditions, treatments, organ transplants, or HIV infection—have an increased risk.
- Rosacea: A 2024 study found that in Caucasians, rosacea is associated with an increased risk of melanoma.
- Previous Cancers: People who have previously had melanoma are at higher risk of developing another primary melanoma. Having nonmelanoma skin cancer, breast cancer, or thyroid cancer also increases risk. Chronic lymphocytic leukemia is also linked to a higher risk—especially within the first five years after diagnosis—likely because it weakens the immune system.
- Obesity: Being overweight or obese is linked to a higher risk of malignant melanoma in men.
- Dermoscopy: Using a dermatoscope—a magnifying lens with a light—the dermatologist can see structures beneath the skin’s surface that aren’t visible to the naked eye.
- Reflectance Confocal Microscopy: This noninvasive technique uses a low-powered laser to create detailed 3D images of suspicious skin areas. It is especially useful for people with many atypical moles because it can reduce unnecessary biopsies and help define the edges of a melanoma before surgery.
- Handheld Spectroscopic Devices: These devices analyze how different wavelengths of light reflect from the skin to help determine whether a spot may be melanoma.
- Adhesive Patch Testing: A sticky patch collects skin cells from a suspicious area. The cells are then tested for gene changes commonly associated with melanoma.
- Skin Biopsy: A sample of skin is removed and examined under a microscope. The type of biopsy—such as excisional, punch, or shave—depends on the size and location of the suspicious area.
If melanoma is confirmed, your dermatologist may recommend more tests to check nearby lymph nodes. These tests are usually based on how deeply the melanoma has penetrated the skin and whether the lymph nodes appear enlarged. They include:
- Sentinel Lymph Node Biopsy: This test examines the lymph nodes closest to the melanoma and can detect very small amounts of cancer spread, even when the nodes do not appear swollen.
- Ultrasound Scan: This imaging test uses sound waves to create images of lymph nodes.
- Fine Needle Aspiration: If an ultrasound identifies an abnormal lymph node, the dermatologist may use a thin needle to remove a small sample of cells. The sample is then examined under a microscope for melanoma cells.
1. Conventional Treatments
Standard treatment for melanoma focuses on removing the cancer and reducing the risk of recurrence or spread.
- Excisional Surgery: Wide local excision is the main treatment for stages 0 and 1 melanoma and is often sufficient on its own. The surgeon removes the tumor along with a margin of healthy tissue, which is then analyzed in a laboratory. If cancer cells are found at the edges, additional surgery may be needed.
- Mohs Micrographic Surgery: Under select circumstances—such as cosmetically sensitive areas—the surgeon removes the tumor in stages, examining each layer under a microscope and removing additional tissue only where cancer cells remain.
If a large amount of skin is removed during melanoma surgery, a skin graft may be performed during the same operation. Healthy skin is taken from another part of the body, like the thigh, and used to cover the surgical site and reduce scarring.
- Imiquimod Cream: A topical treatment that stimulates the immune system by triggering cytokines, including interferon, to help destroy cancer cells.
- Radiation Therapy: A localized treatment that uses high-energy X-ray beams to destroy tumor cells or prevent their growth. Although melanoma is generally less sensitive to radiation than many other cancers, radiation therapy may be used when surgery is not possible or for specific subtypes, such as lentiginous, mucosal, or ocular melanoma.
Stage 2 (Localized but Higher Risk)
- Wide Excisional Surgery: Removal of the primary tumor with appropriate margins.
- Sentinel Lymph Node Biopsy: Often performed at the time of surgery to check for microscopic spread.
Additional Treatment
- Immunotherapy: Enhances the body’s immune response against melanoma. Immunotherapy can be effective on its own or when combined with other treatments. Different types of immunotherapy are used in stage 2 melanoma treatment. Immune checkpoint inhibitors “unmask” cancer by removing the chemical brakes that prevent the immune system from attacking cancer. Oncolytic virus therapy uses a genetically modified virus to kill cancer cells directly while stimulating an immune response.
- Radiation Therapy: May be used at the surgical site after tumor removal to destroy any remaining cancer cells.
Stage 3 (Regional Spread to Lymph Nodes)
- Immunotherapy: Often used after surgery to reduce recurrence risk.
- Targeted Therapy: Designed for tumors with specific genetic mutations. These drugs attack cancer cells with minimal harm to healthy cells and block abnormal proteins that drive tumor growth.
- Oncolytic Virus Therapy: Talimogene laherparepvec, a modified herpesvirus, is injected directly into tumors to destroy cancer cells and stimulate immune activity.
- Chemotherapy: Uses drugs that kill all rapidly dividing cells. It has not been shown to extend survival when used alone in melanoma patients and can cause serious side effects. A regional technique called hyperthermic isolated limb perfusion delivers heated, high-dose anticancer drugs directly to an affected arm or leg by temporarily isolating its blood flow.
Stage 4 (Metastatic Melanoma)
- PD-1 Blockers: Target PD-1 receptors on T-cells (a type of immune cell), allowing the immune system to attack cancer more effectively.
- Combination Immunotherapy: Drug combinations such as nivolumab and ipilimumab or nivolumab and relatlimab enhance immune response and improve survival but may cause more severe side effects.
- Tumor-Derived Autologous T Cell Therapy (Lifileucel): Uses a patient’s own tumor-fighting immune cells, grows them in the lab, and infuses them back into the body to attack melanoma. Typically used after other immunotherapies have failed.
Other treatments include:
- Targeted Therapy: Used for tumors with genetic mutations, such as BRAF. These treatments combine a BRAF inhibitor and a MEK inhibitor to slow tumor growth, prolong response, and reduce certain side effects compared with single-drug therapy.
- Chemotherapy: Now reserved for cases in which immunotherapy and targeted therapy are ineffective or cannot be used.
2. Recurrent Melanoma Treatments
Treatment depends on where the melanoma returns, prior therapies, overall health, and patient preferences.
- Local Recurrence (Near the Original Site): Treated primarily with surgery, sometimes combined with sentinel lymph node biopsy and additional therapy based on findings.
- In-Transit Recurrence (In Nearby Lymph Vessels Under the Skin): Managed with surgery when possible, or with radiation, imiquimod cream, isolated limb chemotherapy, targeted therapy, immunotherapy, or chemotherapy.
- Nearby Lymph Node Recurrence: Treated with lymph node removal, sometimes followed by radiation, immunotherapy, or targeted therapy. If surgery isn’t possible, systemic therapy is used.
- Distant Recurrence: Managed similarly to stage 4 melanoma with systemic therapy, surgery (for isolated tumors), or specialized radiation—particularly for brain metastases.
3. Emerging and Complementary Treatments
Several emerging treatments are under investigation and require further clinical trials to confirm their effectiveness.
- Mistletoe Extract: Used widely in Europe as a complementary cancer therapy. It may act as an antioxidant, reduce inflammation, and slow abnormal cell growth. Up to 77 percent of cancer patients in German-speaking countries report using mistletoe extracts to help slow tumor growth. In two case studies, mistletoe extracts achieved complete remission of melanoma metastases.
- Targeted Nutrient Deprivation: A novel cancer therapy that exploits cancer cells’ reliance on specific amino acids. By limiting access to these nutrients, the therapy aims to weaken tumor cells and enhance other treatments. In a phase I study, a 65-year-old patient with advanced melanoma resistant to prior immunotherapies achieved complete remission lasting more than 30 months.
- Nano-Formulated Natural Compounds: Plant-derived substances such as ginseng, Pistacia lentiscus (mastic tree), and Amaranthus hypochondriacus (Prince’s-feather) are being explored. Nanotechnology—such as liposomes (microscopic fat-based carriers) and nanoemulsions (tiny droplets of oil and water)—may improve drug delivery and absorption.
1. Self-Care Strategies
Though it sounds cliché, the following self-care tips may improve recovery and overall quality of life during and after treatment.
- Prioritize sleep
- Reduce stress
- Stay hydrated
- Choose mild foods if experiencing vomiting or diarrhea
- Avoid smoking
2. Nutrition
Diet may influence treatment response and overall strength.
- Eat a High-Fiber Diet: Fiber may enhance response to immunotherapy by supporting a healthy gut microbiome.
- Prioritize Protein and Nutrient-Dense Foods: When appetite is low, focus on calorie-rich, nutrient-dense foods to maintain weight and strength.
- Include Omega-3 Fatty Acids: Fatty fish, flaxseeds, and chia seeds provide anti-inflammatory support.
3. Mind-Body Practices
Many people use mind-body approaches alongside standard treatment to help manage symptoms and stress.
- Acupressure: May help relieve pain and other physical discomfort. (Acupuncture may have a greater effect, but it requires a trained acupuncturist.)
- Meditation, Yoga, and Breathing Exercises: Can promote relaxation and reduce stress.
- Massage and Biofeedback: Can decrease muscle tension and pain.
Discuss any complementary therapy with your health care provider to ensure it is safe and coordinated with your treatment plan.
- Avoid Excessive Sun Exposure: Sunlight and skin cancer have long been debated—especially given that sunlight may offer protective effects against certain cancers and provide important benefits for overall skin health. The key is moderation and recognizing that each person’s body responds differently.
Generally, limit time in direct sunlight during peak hours—between 11 a.m. and 3 p.m.—when UV rays are strongest. Sunscreen is often recommended; however, its ingredients have come under scrutiny in recent years, especially with daily, all-day use. However, prolonged sun exposure without sunscreen protection, such as during a beach day, can lead to sunburn. Mineral-based sunscreens are a better option for sensitive skin.
Besides, wearing wide-brimmed hats, long-sleeved shirts, and long pants when you are under intense sun for a long time can also be beneficial. Staying in the shade also helps. Sun-protective clothing may list a UV protection factor (UPF) rating from 15 to 50+, with higher numbers offering greater protection. Some laundry detergents can also increase a garment’s UPF. - Avoid Artificial Tanning: Do not use sunlamps or tanning beds.
- Protect Your Immune System: A weakened immune system increases melanoma risk. HIV infection can also impair immunity, so avoiding high-risk exposures, such as intravenous drug use, can help reduce risk.
Evidence for dietary prevention strategies is mixed, and findings should be interpreted cautiously.
- Drink Coffee: A 2017 study suggested that men who drank more coffee had a lower risk of melanoma, possibly due to caffeine, but no clear link was found in women, and later studies have shown mixed results.
- Eat a Healthy Diet: Mediterranean and DASH-Style Eating Patterns have been associated with lower melanoma risk. Some research has found an association between higher red meat intake and a lower risk of melanoma. However, processed meats are linked to other health risks and should be limited.
- Monitor Retinol Intake: Retinol, a form of vitamin A found in animal-based foods, has been linked to a 20 percent lower risk of melanoma.
- Get Adequate Vitamin D: A 2023 study of nearly 500 adults found that consistent use of vitamin D supplements was associated with a lower melanoma risk.