It was 1989, and she was still a resident anesthesiologist, Dr. Heidi Klessig recalled in her book, “The Brain Death Fallacy.”
One day, her attending anesthesiologist told her to prepare a brain-dead organ donor for organ removal surgery.
Upon examining the patient, Dr. Klessig was surprised to find that the man looked exactly like every other critically ill, living patient and, in fact, better than most.
“He was warm, his heart was beating, and his monitors showed stable vital signs,” Dr. Klessig wrote. “Nevertheless, on his bedside exam, he checked all the boxes for brain death, and the neurologist declared him ‘dead.’”
Dr. Klessig’s supervising attending anesthesiologist asked her what anesthesia she was going to give the donor for the operation.
Her answer was a paralyzing agent so the donor wouldn’t move during surgery, as well as some fentanyl to blunt the body’s responses to pain.
The anesthesiologist looked at her and asked, “Well, are you going to give anything to block consciousness?”

Dr. Heidi Klessig in the 1990s. (Courtesy of Dr. Heidi Klessig)
Dr. Klessig was stunned. Consciousness blockers are given to patients to ensure they aren’t awake and aware during an operation.
Her education told her that brain-dead patients should not be conscious; apart from having a biologically active body, their minds were gone.
“I looked at him and said, ‘Why would I do that? Isn’t he dead?’”
Her attending anesthesiologist looked at her and asked, “Why don’t you give him something to block consciousness—just in case.”
“I get a pit in my stomach every time I remember his face,” Dr. Klessig told The Epoch Times. “I remember him looking at me over his mask ... It seemed very confusing.
“I did as I was told, and I’m very grateful [that I did.]”
Is Brain Dead, Dead?
Once a person is brain dead, they become legally dead, but their bodies are technically still alive.
The definition of brain death, also known as death by neurological criteria, is when a person falls into a permanent coma, loses their brainstem reflexes and consciousness, and can’t breathe without stimulus or support.
Yet a person’s heart can be beating, his or her organs functional, and he or she can fight off infection, grow, and even carry babies to term.
Though they may exhibit no signs of consciousness, some areas of the brain may still work. About 50 percent of brain-death patients retain activity in their hypothalamus, which coordinates the body’s endocrine system and regulates body temperature.
However, all of this stops if they are taken off life support.
For this reason, physicians hotly contest whether brain death is synonymous with death.
Dr. James Bernat, a neurologist and professor emeritus at the Dartmouth Geisel School of Medicine, told The Epoch Times that people who are brain dead are dead because their bodies “no longer function as an organism as a whole.” Without the technology to develop these life support machines, these people would be dead, he said.
Radiologist Dr. Joseph Eble and previous academic hematopathologist Dr. Doyen Nguyen, on the other hand, wrote in an article that machines can only sustain life, not generate it—much like how a dead man couldn’t breathe while on a ventilator.
Another topic regarding brain death is whether a patient can still feel.
Among European anesthesiologists, there is an ongoing debate about whether brain-dead organ donors should be given consciousness blockers during organ procurement.
Some argue that they should do so in case patients feel pain. Others disagree. Surprisingly, the anesthesiologists’ position is “not based on the claim that patients were incapable of experiencing pain,” but, instead, out of concern that the public might have doubts about the brain-death diagnosis, bioethicists Dr. Robert Truog and Franklin Miller (who has a doctorate in philosophy) wrote in their book, “Death, Dying, and Organ Transplantation.”
Dr. Ronald Dworkin, a research fellow and anesthesiologist, wrote in an article on organ procurement that he chose to give consciousness blockers because he thought his patient “might still be a ‘little alive’, [sic] whatever that means.”
Mr. Miller, who is also a professor of medical ethics in medicine at Weill Cornell Medical College, said the label of brain death is misleading. He and Dr. Truog, professor of anesthesiology and director emeritus of the Harvard Medical School Center for Bioethics, are of the opinion that brain-dead people are alive but likely will not regain consciousness and recover.
Some say brain-dead patients might actually recover, as in the famous case of Jahi McMath, a 13-year-old girl who was declared brain-dead on Dec. 12, 2013. Her mother opposed her brain-death diagnosis and kept Jahi on life support for 4 1/2 years. Though Jahi could not speak and never regained full consciousness, two neurologists testified that in her final days that she was in a “minimally conscious state.”
Jahi would move to instructions, nurses and doctors testified. Later, an electroencephalogram (EEG) detected brain wave signals.
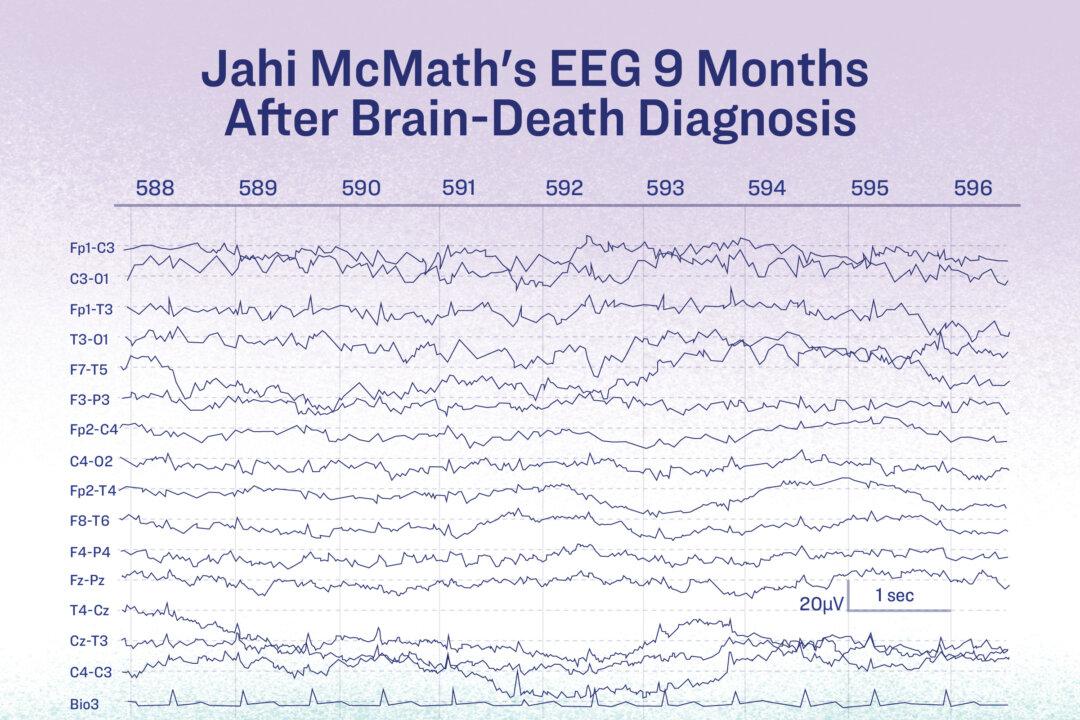
The EEG of Jahi McMath, who was declared brain dead, should have shown no activity. (Illustration by The Epoch Times)
A brain-dead person should have no EEG activity whatsoever.
“Jahi McMath is the sterling example of someone ‘correctly/properly’ diagnosed as being brain dead who subsequently was documented to have recovered brain function,” Dr. Klessig said. The girl was indisputably diagnosed brain dead according to the guidelines of her time and would be diagnosed as such under the new guidelines, she added.
How Is Brain Death Assessed?
According to the most recent brain-death assessment guidelines, published by the American Academy of Neurology (AAN) in 2023, brain death is determined through a bedside assessment.
Before the brain-death assessment is conducted, neuroimaging must be done to ensure there is damage to the brain.
“If you see a normal CAT scan or a normal MRI, then you need to be very, very careful and cognizant that you may be going to a false-positive situation,” Dr. Panayiotis Varelas, one of the co-authors of AAN’s 2010 guidelines and chair of the Department of Neurology at Albany Medical College, told The Epoch Times.
After brain injury is confirmed, two doctors then complete the brain-death assessment. The patient is tested twice for their responsiveness to pain stimulus and brainstem reflexes, with a 24-hour interval between each test.
If the patient tests positive both times, the doctors will conduct an apnea test—considered the most conclusive—to see if the person has lost breathing reflexes. In children, there are two apnea tests, one after each bedside brain-death assessment.
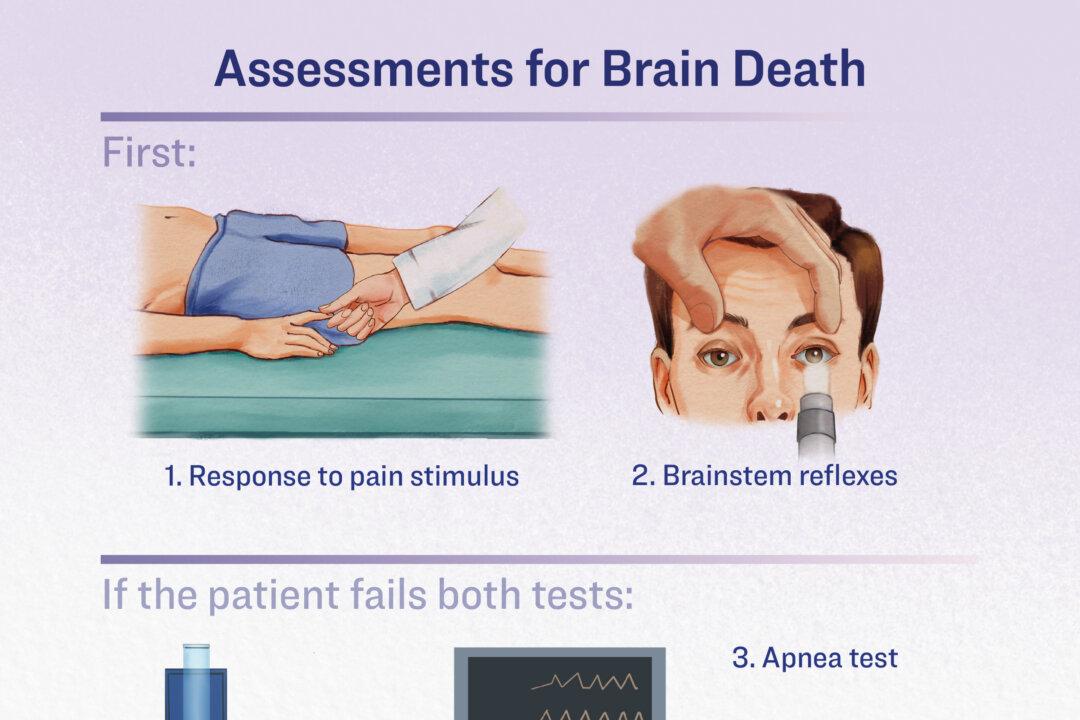
To assess brain death, doctors use a pain stimulus, check for brainstem reflexes, then conduct an apnea test if the patient fails both tests. (Illustration by The Epoch Times)
During the apnea test, the patient is taken off the ventilator for 10 minutes. A tube carrying pure oxygen is inserted into the airways. If the patient does not breathe voluntarily, they are considered brain dead.
The apnea test comes with several risks.
For example, those with respiratory failure may experience complications, including severe hypotension, hypoxia, and cardiac arrhythmia.
In a patient whose brain is already compromised, an apnea test may worsen the person’s condition or cause further damage, Dr. Paul Byrne, regarded as a pioneer in neonatology and involved in treating supposedly brain-dead neonates, told The Epoch Times. A worse condition can compound a brain-death diagnosis in individuals who may actually be on track for recovery.
Misdiagnosis could also occur during brain-death assessment.
One example is Zack Dunlap. In November 2007, he was in a traffic accident and was pronounced brain dead at the hospital.

Zack Dunlap unconscious in the hospital. (Courtesy of Zack Dunlap)
Mr. Dunlap told The Epoch Times that he regained consciousness in the hospital after he was pronounced brain dead and his friends and family were saying their goodbyes.
He tried to scream and move, but nothing happened. Since he was an organ donor, he was soon scheduled for organ procurement.
The family prayed for Mr. Dunlap in the hospital. Mr. Dunlap’s cousin, who is a nurse, didn’t believe it was his time.

Zack Dunlap recovering in the hospital. (Courtesy of Zack Dunlap)
The cousin conducted additional tests on him. When the cousin pressed under Mr. Dunlap’s thumbnail, Mr. Dunlap pulled his arm to the other side of the body. This movement revoked the diagnosis.
After a few more days, Mr. Dunlap began breathing on his own. He was discharged a month later.
Dr. Varelas, who reviewed media reports on Mr. Dunlap, told The Epoch Times that Mr. Dunlap’s outcomes looked so good that he suspects some steps may have been missed during the assessment.
If doctors had adequate experience with brain-death assessments and diligently followed the AAN’s guidelines, false positives would not occur, Dr. Varelas said.
While his hospital makes 50 to 60 brain-death assessments every year, smaller community hospitals may make very few. Therefore, doctors at these hospitals may not have enough experience, miss signs, or carry out the brain-death assessments out of order, he added.
Dr. Bernat said that the test often performed incorrectly is the apnea test.
In 2010, neurologists conducted a review for the AAN to evaluate all cases of recovery from brain death in adults between 1996 and 2009. They determined that there were “no published reports of recovery” from brain death if patients were diagnosed correctly using the brain-death diagnostic criteria of the time. Mr. Dunlap’s case was not assessed.
To further complicate matters, several conditions can mimic brain death. These must be excluded before starting brain-death assessments.
Deceptive Death Conditions
The authors of the 2023 AAN guidelines advise that prior to a brain-death assessment, all of the following conditions should be eliminated, including:
- Hypothermia (low body temperature)
- Autoimmune nervous system diseases
- Drug overdoses
- Poisoning
Therapeutic hypothermia, a treatment that lowers body temperature, is commonly used in patients who have been resuscitated after a cardiac arrest. Cooling devices are applied to help the body and brain recover and heal. However, hypothermic patients can take up to a week to regain consciousness.
Autoimmune conditions such as Guillain-Barré syndrome, which damages a person’s nervous system, can also rob someone of their reflexes and consciousness.
Dr. May Kim-Tenser, associate professor of clinical neurology at Keck School of Medicine at the University of Southern California, reported in 2016 on a case in which a patient with a form of Guillain-Barré syndrome was initially misdiagnosed as brain dead.
The patient was admitted to the hospital after showing severe symptoms. Within several days, he became unconscious and unresponsive, lost his brainstem reflexes, and needed a ventilator to breathe.
An apnea test was not conducted. Had the patient been tested in such a way, he would have failed because he would have been too weak to breathe, Dr. Kim-Tenser said.
The patient was then transferred to Dr. Kim-Tenser’s hospital, where he was prescribed autoimmune disease medication. Later, he regained consciousness and some function of his limbs.
Drug overdoses from opioids and cocaine can also cause signs of brain death. An overdose on the muscle relaxant baclofen, for instance, has been known to mimic brain death.
“The brain death guidelines talk about what the mimickers are but not necessarily ways to exclude them. A neurologist should be able to exclude them with testing,” Dr. Kim-Tenser said.
Potential Conflicts of Interest
“There is an intense interest in [brain death] by [organ-procurement organizations], the transplantation community, and patients on organ-waiting lists,” Dr. Varelas wrote in a 2016 article on brain death.
Around 90 percent of all organ donors are brain-dead people. This is because the brain-death definition allows surgeons to procure healthy organs without invoking the “dead-donor rule.”
According to the dead-donor rule, an ethical norm, organ donors must be declared dead before organ procurement, and organ procurement must not cause the donor’s death.
Organs cannot be transplanted from people who are biologically dead, which occurs after a person’s heart stops and he or she cannot be resuscitated.
“When you’re biologically dead, the loss of oxygen to your vital organs causes them to decompose so quickly that you cannot donate an organ,” Dr. Klessig said.
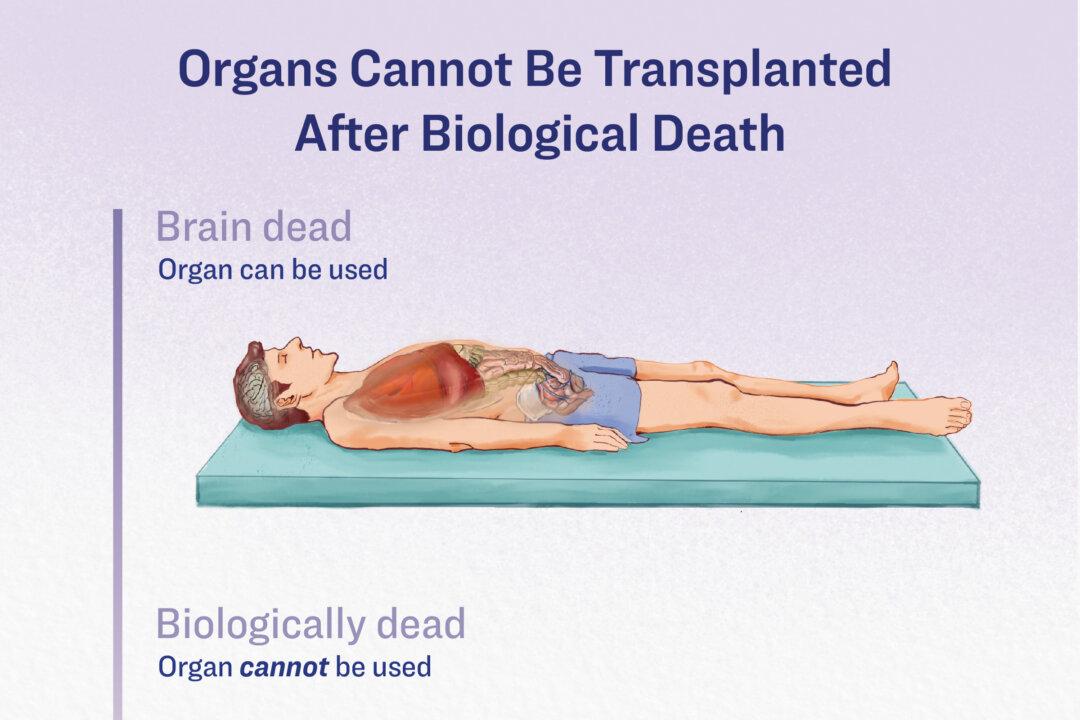
Once a person is biologically dead, their organs cannot be harvested for donation. (Illustration by The Epoch Times)
That said, tissues such as cornea, cartilage, bone, and skin can come from dead donors. Live-organ donation can also be done to transplant the lobe of a lung, liver, or kidney.
Doctors who make brain-death assessments must not be involved in the organ procurement process.
“We try to disassociate ourselves from the organ-donation process,” Dr. Varelas said. “In my mind, we try to save the patient’s life, and that’s the goal because the Hippocratic Oath is to do no harm.”
Synonymizing brain death with death is an issue of non-transparency, Mr. Miller said. However, he said he would not consider organ procurement unethical as long as the donor is well informed.
In the United States, many people sign up to become organ donors when they apply for a driver’s license, and most of them assume that their organs will only be removed in the case of their death, Dr. Klessig said.
“They think, ‘If I’m as good as done, might as well take my organs anyway,’” Dr. Byrne said.
The reality is that their donor status can result in their organs being procured if they become “brain dead,” with their family members unable to override donor status.
Still a Mystery
The concept of brain death started more than half a century ago, a few years after the first organ transplant was successfully performed.
Organ procurement from comatose people started in the late 1950s. However, this was rare and not practiced under any guidelines. During the same era came a shift in the definition of death.
In 1959, French doctors Pierre Mollaret and Maurice Goulon coined the term “le coma dépassé,“ meaning ”beyond coma“ or ”irreversible coma,“ as a condition synonymous with death. Gradually, brain death, also called ”death of the nervous system,” became a new definition, and organs could, therefore, be procured from such patients.
On Dec. 3, 1967, the world was astounded by the first report of a successful human heart transplantation performed by Dr. Christiaan Barnard in Cape Town, South Africa. The heart was procured from a trauma victim with massive head injuries. The donor had no brain activity detected on EEG scans and lacked brainstem reflexes. However, her heart continued to beat with life support.
The heart recipient survived for 18 days before succumbing to pneumonia, but his heart functioned properly until his death. This success initiated the practice of heart transplantation.
A month after Dr. Barnard’s monumental surgery, Dr. Norman Shumway performed the first human heart transplant in the United States at Stanford Hospital, removing the heart from a brain-dead donor.
The chief resident assisting him asked, “Do you think this is really legal?”
“I guess we'll see,” Dr. Shumway said.
In August 1968, the Ad Hoc Committee of Harvard Medical School published “A Definition of Irreversible Coma” in the Journal of the American Medical Association.
They defined irreversible coma as a “new criterion for death,” which has become a foundational cornerstone to the brain-death definition.
Despite this, scientists are still uncertain whether the definition or the consequent assessment is perfect.
Regarding Mr. Dunlap’s recovery, Dr. Varelas said, “I am glad this young man survived.” He believes the family’s prayers for Mr. Dunlap could have contributed to his outcome.
“There are powers much higher than our medical knowledge—or the lack thereof,” he said.
“The secret of life—including the definition of life—still remains the deepest and most mysterious one,” Dr. Dworkins said.
He added that nature may never “permit anyone to know the exact point where brain death becomes real death.”